Pharmacology: AA Pharma Nifedipine is a calcium ion influx inhibitor (calcium entry blocker or calcium ion antagonist). The anti-anginal effect of this group of drugs, is believed to be related to their specific cellular action of selectively inhibiting transmembrane influx of calcium ions into cardiac muscle, and vascular smooth muscle. The contractile processes of these tissues are dependent upon the movement of extra-cellular calcium into the cells through specific ion channels.
Nifedipine blocks the transmembrane influx of calcium through the slow channel without affecting to any significant degree the transmembrane influx of sodium through the fast channel. This results in a reduction of free calcium ions available within cells of the above tissues. Nifedipine does not alter total serum calcium.
The specific mechanisms by which nifedipine relieves angina has not been fully determined but it is believed to be brought about largely by its vasodilatory action.
Nifedipine dilates the main coronary arteries and coronary arterioles both in normal and ischemic regions and is potent inhibitor of coronary artery spasm. This property increases myocardial oxygen delivery and is responsible for the effectiveness of nifedipine in vasospastic angina.
Nifedipine by its vasodilatory action on peripheral arterioles, reduces the total peripheral vascular resistance. This reduces the workload of the heart and thus reduces the myocardial energy consumption and oxygen requirements and probably accounts for the effectiveness of nifedipine in chronic stable angina.
The negative inotropic effect of nifedipine is usually not of major clinical significance because the drug's vasodilating properties evoke at therapeutic doses a baroreceptor-mediated reflex tachycardia which tends to counterbalance this negative inotropic effect.
At the usual therapeutic doses nifedipine does not possess antiarrhythmic properties.
In man, oral administration of 10 mg C14 nifedipine resulted in more than 90% absorption of the drug. Radioactivity was detectable in the serum 20 minutes after oral ingestion and peak serum levels were reached in 1 to 2 hours. 70 to 80% of the activity was eliminated via the kidneys and the remainder via the feces.
The bi-exponential analysis of the disappearance of nifedipine in the plasma yields an initial fast half-life (T1/2) of 2.5 to 3 hours and a terminal slow half-life (T1/2) of 5 hours.
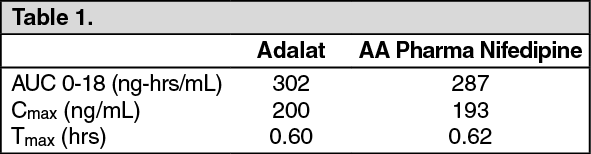
A comparative bioavailability study was performed on Adalat 10 mg Capsules vs. AA Pharma Nifedipine 10 mg Capsules using 24 (twenty-four) normal volunteers. A single dose of 20 mg was administered. The results are as follows: (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Studies in man, dog and rat showed that nifedipine is almost completely metabolized in the body. It is transformed into two pharmacologically inactive metabolities. The main metabolite is the hydroxycarboxylic acid derivative which represents about 95%, the other is the corresponding lactone, which represents about 5%. The acid form is mainly excreted in the urine. Protein binding of circulating nifedipine exceeds 90%.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
